Acromioclavicular Joint Injuries in Rugby
Rugby is a physically demanding sport that subjects players to high-impact collisions, putting their joints, particularly the acromioclavicular (AC) joint, at significant risk. The AC joint, where the clavicle (collarbone) meets the acromion of the scapula (shoulder blade), is crucial for shoulder movement and stability. It is supported by ligaments, including the acromioclavicular and coracoclavicular ligaments. In rugby, direct trauma—often from tackles or falls onto the shoulder—can result in AC joint injury. Understanding these injuries, their management, and rehabilitation strategies is key to helping players recover and return to the game safely.
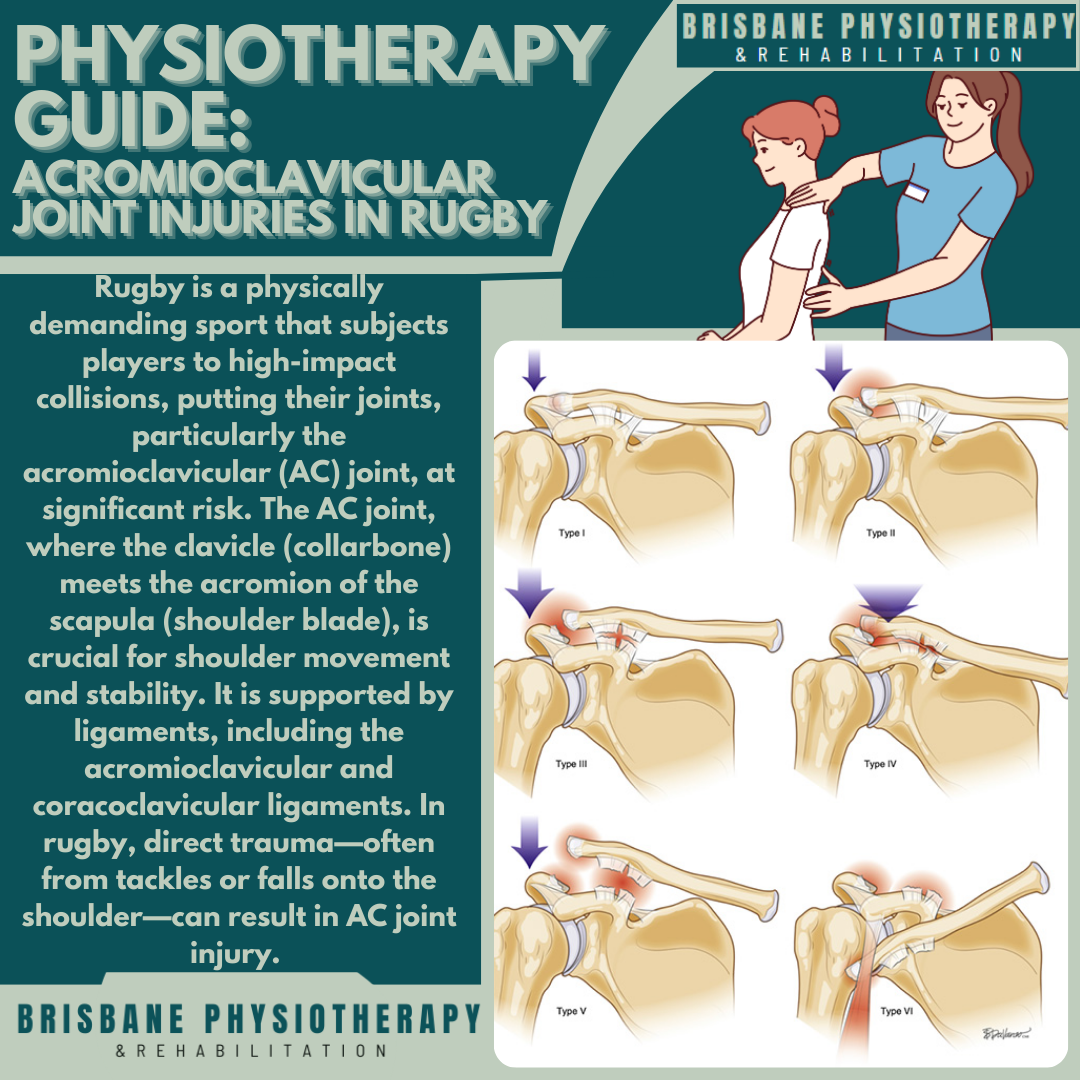
AC joint injuries are graded based on severity:
Grade I: Mild sprain of the AC ligament with minimal pain and swelling.
Grade II: Partial rupture of the AC ligament, possible mild displacement.
Grade III: Complete rupture of the AC and coracoclavicular ligaments, with visible deformity (step deformity).
Grade IV: Posterior displacement of the clavicle into or through the trapezius muscle, often requiring surgery.
Grade V: Severe superior displacement of the clavicle, with a dramatic step deformity due to complete ligament rupture.
Grade VI: Inferior displacement of the clavicle into the subacromial or subcoracoid region, a rare but severe injury requiring urgent surgical intervention.
Mechanism of Injury in Rugby
The most common causes of AC joint injuries in rugby include:
Direct impact: A forceful tackle or a fall directly onto the shoulder.
Repetitive microtrauma: Chronic stress from contact and scrummaging can lead to degenerative changes in the joint.
When is Surgery Needed?
Grades IV–VI injuries often require surgical stabilisation, as they involve significant clavicle displacement. Additionally, players with persistent pain or instability despite conservative treatment may require surgical intervention.
Preventing AC Joint Injuries in Rugby
Proper tackling technique: Encouraging players to use their legs and core instead of leading with the shoulder.
Strength training: Focusing on scapular stability, rotator cuff strengthening, and upper body conditioning.
Protective gear: Wearing padded shoulder supports can provide some protection.
Gradual return to play: Working with physiotherapists and medical staff on a graded return-to-play programme can help reduce re-injury risk.
Final Thoughts
AC joint injuries are common in rugby but can be effectively managed with proper rehabilitation. Physiotherapists play a key role in guiding players through recovery, ensuring a safe and efficient return to sport. With a structured rehab programme and preventive strategies, rugby players can minimise their risk and maintain peak performance on the field.